Research perspective · Ex vivo terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More breast-tissue imaging
Ex Vivo Breast Tumor Identification: Advances Toward a Silicon-Based TerahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More Near-Field Imaging Sensor
Breast-conserving surgery creates a demanding measurement problem: an excised specimen must be examined for tissue boundaries, yet conventional terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More imaging has millimeter-scale resolution at the frequencies most compatible with compact electronics. This article connects two stages of research. First, far-field measurements on freshly excised breast specimens test whether tissue classes produce measurable dielectric contrast in the 300-600 GHz band. Second, the authors discuss a silicon near-field sensor concept intended to overcome diffraction by placing the sample close to an integrated source and detector. The work establishes ex vivo physical contrast and a technology direction; it does not validate clinical diagnosis or an intraoperative medical device.
TerahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More contrast in tissue is strongly influenced by water, lipids, cell density and structural organization. Malignant, fibrous and adipose regions can therefore differ in absorption and refractive index, but those variables are not unique markers of cancer. Freshness, hydration, compression, thickness and sample geometry also affect reflection measurements. Histopathology remains the reference needed to interpret spatial correspondence. The study’s value lies in bringing semiconductor engineering, terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More spectroscopy and pathology into the same measurement chain while keeping the limitations of the far-field experiment visible.
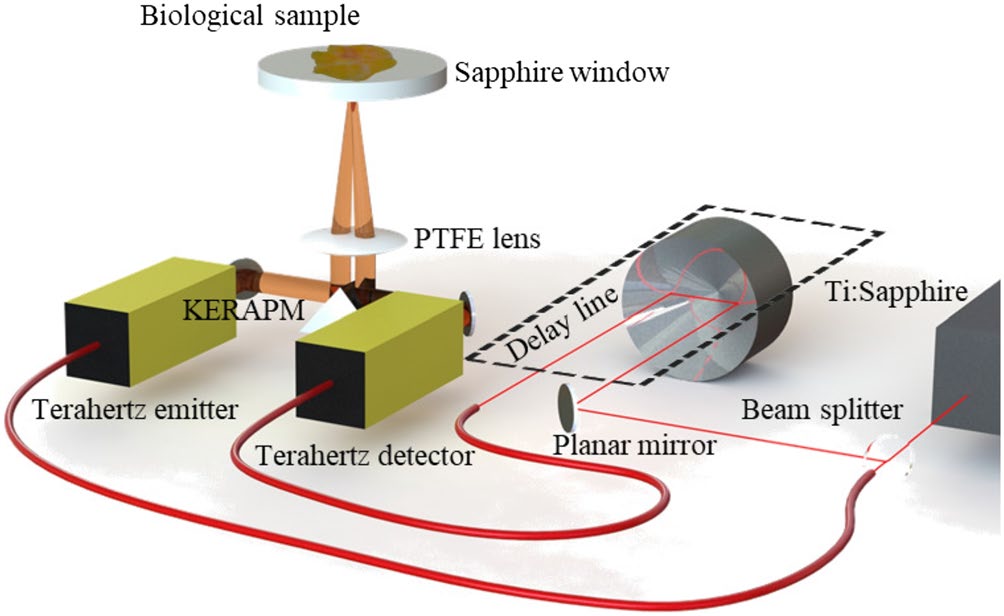
Featured visual: Contextual research figure from âTerahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More refractive index-based morphological dilation for breast carcinoma delineationâ. It illustrates a closely related terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More topic and is not a figure from the publication discussed on this page. Source publication.

Visuals are drawn from the Airtable research archive. Figure numbering, rights and interpretation should be checked against the original publication before republication outside this site.
From ex vivo spectra to an integrated near-field concept
The experimental tissue work used a commercial TeraPulse 4000 time-domain system in reflection. Freshly excised samples were held between two sapphire substrates, each 2 mm thick, to provide a controlled interface. The instrument sampled the specimen with steps between 100 and 500 micrometers. At 300 GHz, however, the effective spatial resolution remained around 1 mm because the free-space wavelength and focusing optics, rather than the mechanical step alone, set the independent detail that could be resolved.
Reflected pulses were detected with a photoconductive antenna and transformed into frequency-domain data. The analysis extracted parameters of a double-Debye dielectric model, allowing the authors to compare frequency-dependent tissue response rather than relying on one image intensity. Images near 500 GHz showed contrast among regions identified as adipose, fibrous or malignant in the associated tissue assessment. The authors also applied principal component analysis to Fourier-amplitude data across 300-600 GHz. The first components summarized correlated spectral variation and highlighted broad tissue structure and boundaries.
PCA is useful here as an exploratory reduction of a multi-frequency data cube, not as a clinically validated classifier. A component can reveal a repeatable direction of variance without proving what biochemical factor causes it. Alignment with histological sections is therefore essential, and performance would need to be measured on a substantially larger, independently tested specimen set before sensitivity or specificity could be claimed.
The semiconductor proposal addresses the mismatch between the observed contrast and far-field resolution. Instead of propagating a beam through conventional optics, a near-field device would integrate a terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More illumination structure, an evanescent-field sensing surface and a power detector in silicon. When tissue is placed within the localized field, spatial detail is governed by the sensor geometry and sample distance rather than by free-space diffraction alone. The article discusses sub-micrometer potential at the device level, but that target should not be confused with the approximately millimeter-scale resolution of the reported far-field tissue maps.
Integration in silicon could make arrays, readout electronics and compact packaging more feasible than a system assembled from separate laboratory components. It also introduces new constraints. The useful near field decays rapidly with distance, so surface contact, flatness and contamination become critical. Strong water absorption limits penetration, and a highly localized surface measurement cannot automatically characterize a margin several millimeters deep. Heating, repeatability, sterilization, sample handling and the relationship between sensor output and histopathology would all require dedicated testing.
Evidence, clinical boundaries and next validation steps
The measurements support a restrained conclusion: freshly excised breast tissues can display different terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More dielectric responses under the study’s controlled reflection protocol. Spectral analysis and PCA provide ways to represent those differences, while the near-field architecture offers a route toward finer surface sampling. They do not show that every malignant region is distinguishable from every benign or normal region, nor that the contrast is independent of hydration, fibrous content or specimen preparation.
Any future medical evaluation would need to define the intended use precisely. Mapping the surface of an excised specimen, estimating the depth of a boundary and diagnosing disease in vivo are different tasks with different evidence requirements. For specimen assessment, researchers would need blinded comparison against spatially registered histopathology, multiple tissue subtypes, benign lesions, treatment effects and realistic handling times. Algorithms would need an independent test cohort and confidence measures, not only visually persuasive component maps.
The paper also places a realistic systems requirement on acquisition time: a potential operating-room workflow cannot wait for slow laboratory scans. A useful platform would need to cover the relevant specimen area, maintain stable contact or controlled spacing, and produce interpretable data within the available procedure window. Those goals involve array design and electronics as much as electromagnetic sensitivity. They also require collaboration with pathologists and surgeons to determine which spatial resolution and depth actually change a decision.
The author team spans silicon terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More circuits, microwave systems, spectroscopy and breast pathology. This multidisciplinary structure is a strength because no single specialty can establish the complete chain from dielectric contrast to clinical utility. Device engineers can improve local field confinement and array readout; spectroscopists can characterize frequency-dependent response; pathology partners can define ground truth and identify confounding tissue structures. Such collaboration should be framed as staged validation rather than a direct path from a promising image to routine surgery.
As a research perspective, the article identifies a productive convergence. Far-field spectroscopy supplies evidence that there is information to measure, and near-field silicon technology addresses the spatial-resolution barrier. The next decisive results would come from an integrated sensor tested on well-characterized ex vivo specimens under a fixed protocol. Until then, the work is best understood as feasibility evidence for tissue contrast and an engineering roadmap, not a claim that terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More imaging detects breast cancer or reduces re-operation rates.
Publication and citation
Recommended citation: Pfeiffer, U. R., Zimmer, T., Hillger, P., Jain, R., Grzyb, J., Bucher, T., Cassar, Q., MacGrogan, G., Guillet, J.-P., & Mounaix, P. (2019). Ex vivo breast tumor identification: Advances toward a silicon-based terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More near-field imaging sensor. IEEE Microwave Magazine, 20(9), 32-46. https://doi.org/10.1109/MMM.2019.2922119
Publisher: IEEE. Airtable record: recgQ0moC1Yw8ULzn.