Research publication · Ex vivo terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More near-field microscopy
TerahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More near-field microscopy of ductal carcinoma in situ (DCIS) of the breast
Ductal carcinoma in situ can form structures only a few hundred micrometres across, far below the millimetre-scale resolution of conventional far-field terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More imaging. This preliminary laboratory study asks whether a localized terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More source can reveal such a lesion in an excised, formalin-fixed and paraffin-embedded human breast tissue specimen. Using a scanning point terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More source microscope, the researchers mapped a focus of DCIS approximately 500 micrometres in diameter in both transmission and reflection. The measured contrast followed differences in tissue architecture and cell packing under the preparation conditions. It establishes microscopic terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More contrast in one processed specimen; it does not validate diagnosis, surgical guidance or performance in fresh tissue.
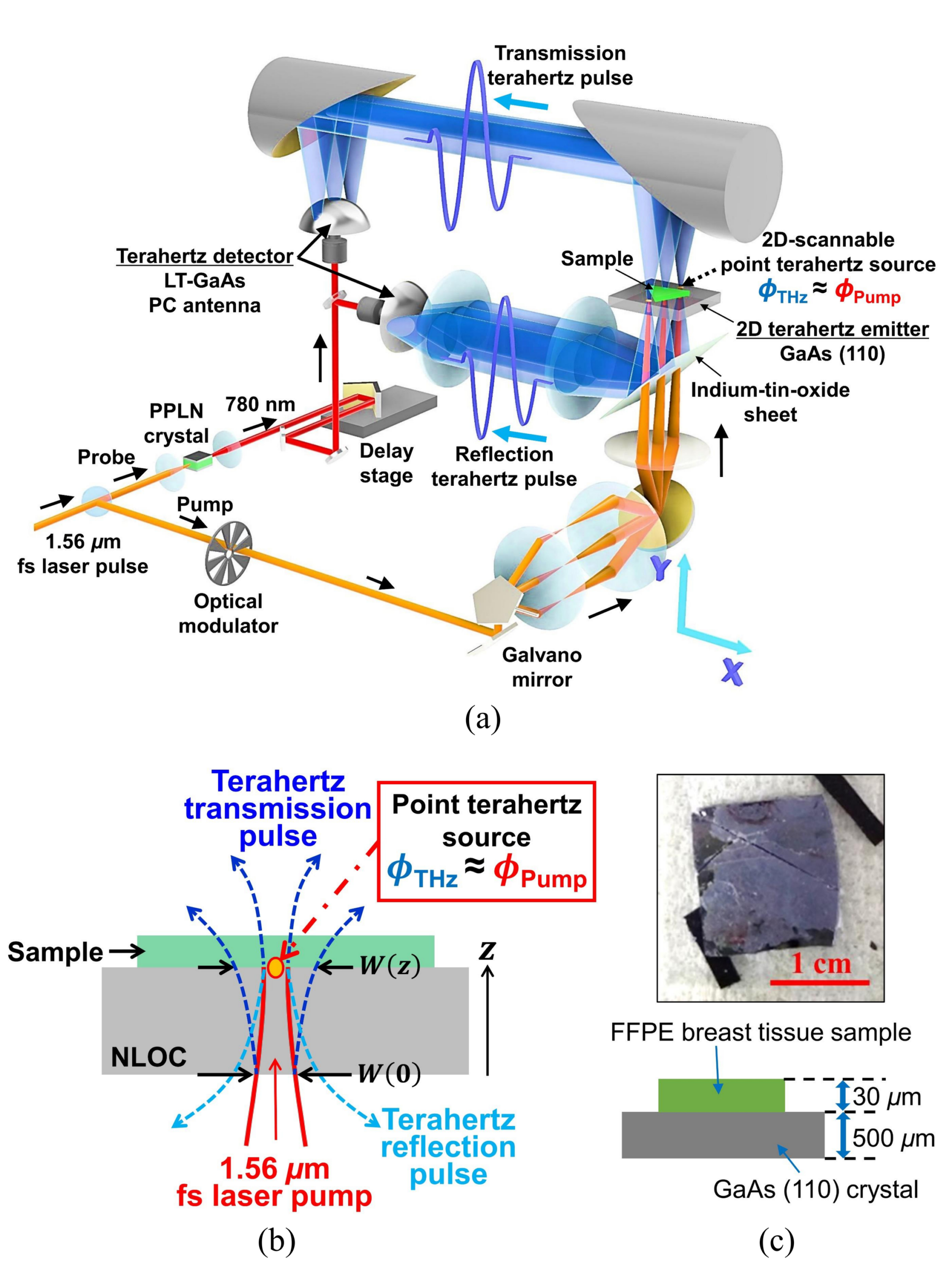
Breast tissue is microscopically heterogeneous. Invasive ductal carcinoma, in situ disease, fibrous stroma and adipose regions may lie close together, and their relative proportions vary over short distances. TerahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More measurements are sensitive to dielectric properties affected by water, composition and structure, but a standard focused beam averages these variations over an area larger than many DCIS ducts. The scanning point terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More source, or SPoTS, microscope addresses the spatial problem by generating the radiation immediately beside the sample. A femtosecond near-infrared pump is focused onto a GaAs crystal; optical rectification produces a terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More source whose lateral extent is governed mainly by the pump spot rather than by free-space focusing of a millimetre wavelength.
The specimen was a 30 micrometre section placed directly on a 500 micrometre GaAs plate. It contained areas identified histologically as invasive ductal carcinoma, DCIS and fibroadipose tissue. A nearby hematoxylin-and-eosin-stained section supplied the pathological reference, so correspondence was based on registration between adjacent tissue information rather than a simultaneous measurement of the same stained plane. Paraffin embedding dehydrates tissue and removes much of its lipid content. That preparation reduces the water-dominated contrast expected in fresh material and makes the experiment useful for investigating structural effects, but it also means the reported amplitudes cannot be carried directly into an intraoperative setting.
Featured visual: Contextual research figure from âScanning point terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More source microscopy of unstained comedo ductal carcinoma in situâ. It illustrates a closely related terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More topic and is not a figure from the publication discussed on this page. Source publication.

Visuals are drawn from the Airtable research archive. Figure numbering, rights and interpretation should be checked against the original publication before republication outside this site.
Creating a microscopic terahertz map without a physical probe
The pump spot was scanned by a galvanometer while a synchronized photoconductive receiver recorded the transmitted or reflected time-domain field. The system could sample with steps as small as 500 nanometres, although sampling pitch is not the same as optical resolution. The experimentally demonstrated spatial resolution was on the order of 20 micrometres, and usable spectral information extended to about 3 THz. A broad 2750 by 1375 micrometre transmission map was first acquired with a 2 micrometre step. The team then examined an 1100 by 825 micrometre region more densely, using the 500 nanometre step to represent the lesion boundary and surrounding structures.
Transmission amplitude was highest in fibroadipose tissue, lower in invasive carcinoma and lowest in the DCIS focus. The localized dark area in the terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More map aligned with the roughly 500 micrometre lesion in the histological reference. Time-domain signals showed the same ordering in peak electric field and a small additional delay, about 0.04 ps, for DCIS. After Fourier transformation, attenuation over approximately 0.5 to 2.5 THz remained greater in DCIS than in invasive carcinoma or fibroadipose tissue. Measurements at several locations reproduced the general trend within this specimen, which supports a real spatial contrast while remaining far short of a population-level sensitivity or specificity estimate.
The authors interpret the higher attenuation in relation to cell density. DCIS ducts in the selected area were densely filled with neoplastic epithelial cells, whereas the invasive region also contained fibrous stroma and the background included more extracellular matrix and adipose structures. Greater nuclear and cellular packing can modify effective dielectric properties and scattering. The experiment does not isolate a single causal variable, however. Uneven paraffin coverage, local thickness, the imperfect match between sections and residual compositional differences can also affect amplitude and phase. The measured signal should therefore be described as tissue contrast correlated with the annotated morphology, not as a molecularly specific signature of DCIS.
Reflection measurements, significance and limits
Reflection is important because thick or water-rich tissue cannot generally be examined in transmission. In the reflective configuration, the microscope measured the pulse returning from the GaAs-tissue interface over an 840 by 840 micrometre area. Both malignant regions produced stronger reflected fields than the surrounding benign tissue, and DCIS showed a slightly larger peak and phase shift than invasive carcinoma at the sampled points. The difference between those two lesions was less pronounced than in transmission, but the location of the DCIS structure remained visible. This agreement between geometries strengthens the physical observation without making reflection-mode performance clinically established.
The work is best understood as a feasibility experiment in near-field biophotonics. It shows that the diffraction limit of conventional terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More imaging is not an absolute barrier to viewing sub-millimetre tissue architecture when the source is generated locally. It also demonstrates rapid electronic-optical scanning without dragging a sharp probe over the specimen. Yet the evidence comes from a processed section and a single complex sample. Histological registration, preparation-induced changes, limited field of view and the need for close contact with the emitter all constrain interpretation. Fresh excised tissue introduces water absorption, surface topography and thickness variations that were largely absent from this protocol.
Any future medical use would require a much broader programme: repeat measurements on independently annotated specimens, blinded evaluation, controlled comparison of fresh and embedded tissue, and an assessment of variation among benign structures, invasive subtypes and DCIS patterns. Instrument engineering would also have to enlarge the field, preserve micrometre-scale resolution, shorten acquisition and provide reproducible sample positioning. Those steps are not demonstrated here. Accordingly, the article supports neither a clinical diagnostic claim nor an assertion that the microscope can determine surgical margins.
The collaboration joined near-field terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More engineering in Japan with breast pathology and terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More analysis expertise in Bordeaux. Its durable contribution is a carefully localized observation: under the stated ex vivo preparation and measurement conditions, a DCIS focus of about half a millimetre generated distinct time-domain and spectral contrast. That result provides a basis for studying how tissue microarchitecture contributes to terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More response and for designing more representative validation experiments, while keeping histopathology as the reference used to identify the lesion.
Bibliographic reference
Recommended citation: Okada, K., Serita, K., Cassar, Q., Murakami, H., MacGrogan, G., Guillet, J.-P., Mounaix, P., & Tonouchi, M. (2020). TerahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More near-field microscopy of ductal carcinoma in situ (DCIS) of the breast. Journal of Physics: Photonics, 2(4), 044008. https://doi.org/10.1088/2515-7647/abbcda
Publisher: IOP Publishing. Airtable record: rec4PA095cDfCj2nB.