This pilot study investigates the dielectric response of freshly excised human breast tissue between 300 and 600 GHz. Its immediate goal is not to claim a clinical diagnostic method, but to determine whether this relatively narrow sub-terahertz window contains measurable contrast that could inform the design of future silicon-based near-field imagers. Histopathology provides the anatomical reference for interpreting the terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More maps.
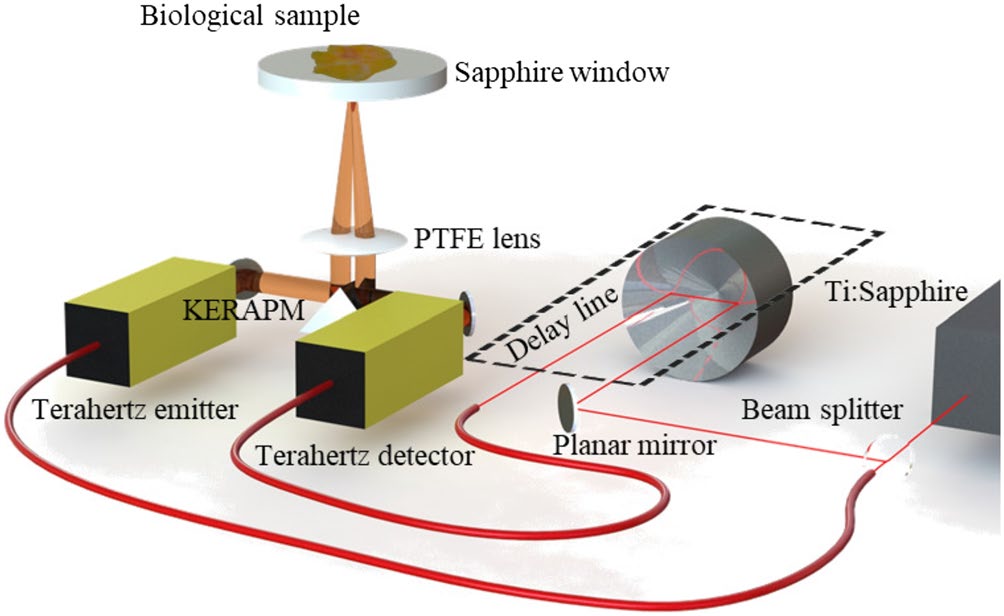
Featured visual: Contextual research figure from âTerahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More refractive index-based morphological dilation for breast carcinoma delineationâ. It illustrates a closely related terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More topic and is not a figure from the publication discussed on this page. Source publication.

Visuals are drawn from the Airtable research archive. Figure numbering, rights and interpretation should be checked against the original publication before republication outside this site.
Fresh-tissue measurements with a pathology reference
Sixteen specimens from eleven patients were measured after breast-conserving surgery, mastectomy or breast reduction. The set included several lesion types and non-malignant tissue. Samples were examined within about 30 minutes of excision to limit changes caused by dehydration and degradation. Each specimen was divided so that one portion could be measured by terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More reflection and the corresponding material could be processed for hematoxylin-and-eosin histology.
The terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More system was a modified TeraPulse 4000 operating in reflection. Broadband pulses generated by a photoconductive antenna were directed through a 2 mm thick C-cut sapphire plate onto the tissue. The temporal record contained a reflection from the air-sapphire boundary and a later reflection from the sapphire-tissue interface. Isolating the second return made it possible to estimate the tissue-dependent complex response while the sapphire provided a stable measurement window.
The scans used lateral steps of either 100 or 500 micrometers according to specimen size and acquisition constraints. The focused beam was approximately 1 mm in diameter, so the pixel step should not be confused with independent spatial resolution. Calibration included baseline removal, phase correction using water-related reference data, temporal windowing and zero-padding before Fourier transformation. The reported uncertainty was around 5 percent for refractive index and 10 percent for absorption coefficient over the broader 0.2-1 THz validation range.
Contrast in the 300-600 GHz window
The analysis compared regions described as adipose, adipose-fibrous and cancerous-fibrous mixtures. Across representative specimens, regions containing cancerous and fibrous tissue generally had a higher effective refractive index than adipose-rich regions, with differences often greater than 0.2. The result appears to reflect tissue composition and hydration rather than a unique spectral signature of a cancer subtype.
Amplitude maps also produced visible contrast because the Fresnel reflection at the sapphire interface depends on the difference between the refractive indices of sapphire and tissue. With sapphire near 3.10, adipose tissue generated a different return from fibrous or malignant-fibrous regions. Boundaries in many terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More maps were reported to agree with corresponding histological regions within fewer than two scan pixels. Uneven tissue contact could distort that contrast, emphasizing that mechanical presentation of the sample is part of the measurement.
The researchers explored principal component analysis on the frequency-dependent amplitude data. In a non-malignant specimen, the first components reproduced major anatomical structure and separated adipose from fibrous regions after non-tissue pixels were excluded. This demonstrates that multivariate processing can organize the measured variation without assigning every pixel manually. It is not a validated automated classifier: the cohort was small, some pixels remained ambiguous and no independent test set was reported.
Water absorption and dielectric relaxation shape the entire band, including behavior near 570 GHz. Consequently, contrast can change with temperature, hydration, contact pressure, tissue thickness and elapsed time after excision. Histological processing also deforms tissue, which complicates pixel-perfect comparison between a fresh specimen and a later stained section. These factors must be controlled before group differences can be turned into robust imaging criteria.
Relevance to terahertz technology and biomedical research
The value of the 300-600 GHz window is partly technological. It can be reached by silicon-germanium BiCMOS circuits, opening a path toward compact arrays and near-field operation rather than a large ultrafast-laser system. Higher frequencies within the band reduce wavelength, while lower frequencies can offer stronger penetration and favorable contrast. The tissue data provide design evidence for exploring that trade-off.
Clinically, the study remains preliminary and ex vivo. It does not report sensitivity, specificity, surgical decision accuracy, recurrence outcomes or a comparison with current margin-assessment standards. It cannot support a claim that terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More imaging detects breast cancer in patients or reduces repeat surgery. Those questions require larger prospective cohorts, pre-specified endpoints, blinded histopathological comparison and a device capable of reproducible whole-margin imaging.
The collaboration joins terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More spectroscopy and electronics groups with pathology and surgical sample access. That combination is a substantive strength because the engineering target was selected from real tissue measurements and checked against histological structure. The cautious conclusion is that measurable dielectric differences exist in freshly excised specimens and that the selected band merits further instrument development.
Future research would need faster arrays, improved contact control, repeated measurements across tissue temperature and hydration, and classification models tested on unseen cases. Within its pilot scope, the paper provides a careful bridge between broadband biomedicalTerahertz and millimeter-wave technologies offer promising non-ionizing tools for biomedical tissue analysis, particularly for breast cancer research. Their sensitivity to water content, tissue structure, and dielectric contrast can help distinguish... More spectroscopy and the requirements of a future sub-terahertz imaging sensor.
Publication details and citation
Recommended citation: Cassar, Q., Al-Ibadi, A., Mavarani, L., Hillger, P., Grzyb, J., MacGrogan, G., Zimmer, T., Pfeiffer, U. R., Guillet, J.-P., & Mounaix, P. (2018). Pilot study of freshly excised breast tissue response in the 300-600 GHz range. BiomedicalTerahertz and millimeter-wave technologies offer promising non-ionizing tools for biomedical tissue analysis, particularly for breast cancer research. Their sensitivity to water content, tissue structure, and dielectric contrast can help distinguish... More Optics Express, 9(7), 2930. https://doi.org/10.1364/BOE.9.002930
Record ID: recJ9G9bRGXhyoM5M
Research themes: ex vivo breast tissue, dielectric contrast, THz-TDS, 300-600 GHz imaging, histopathology comparison, biomedicalTerahertz and millimeter-wave technologies offer promising non-ionizing tools for biomedical tissue analysis, particularly for breast cancer research. Their sensitivity to water content, tissue structure, and dielectric contrast can help distinguish... More terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More research.