Research publication · Ex vivo terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More tissue analysis
TerahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More refractive index-based morphological dilation for breast carcinoma delineation
This exploratory study combines a physical measurement with a simple image-processing operation. Refractive-index maps were derived from reflected terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More pulses acquired on three freshly excised human breast specimens, then thresholded and morphologically dilated to classify pixels against histopathology-derived annotations. For the best-performing specimen and configuration, the reported sensitivity was about 80% and specificity about 82%; results were weaker for the other specimens, particularly an invasive lobular carcinoma. The experiment shows how spatial processing can compensate partly for diffuse contrast and limited resolution in a small ex vivo data set. It does not establish a clinically validated margin-assessment system, and its performance cannot be generalized beyond the tested tissues.
The rationale begins with a mismatch between biological boundaries and instrument response. A tumour does not necessarily form a uniform block of malignant cells, and a focused terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More beam averages tissue properties over a finite spot. Thresholding a refractive-index map pixel by pixel can consequently leave gaps within a histological tumour region. Morphological dilation expands each positive pixel into a defined neighbourhood. In this context it is a deliberate hypothesis: a high-index measurement may indicate malignant tissue whose extent is broader than the isolated pixel suggests. Expansion can recover missed tumour area, but it can also relabel adjacent benign tissue and reduce specificity.
The specimens came from three excisions: two invasive ductal carcinomas and one invasive lobular carcinoma. They were maintained in physiological serum and measured within approximately one hour to limit changes in hydration and tissue condition. This was an ex vivo protocol, not an in vivo or intraoperative trial. After terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More acquisition, standard histological processing supplied the reference maps. Fixation, dehydration, sectioning and differences between the measured surface and the microscopic section can deform the tissue, making image registration itself a significant source of uncertainty.
Featured visual: Image 1 from the Airtable record associated with this publication. Consult the original paper for the authoritative figure caption and interpretation. Source publication.
Visuals are drawn from the Airtable research archive. Figure numbering, rights and interpretation should be checked against the original publication before republication outside this site.
Building and expanding a 550 GHz refractive-index map
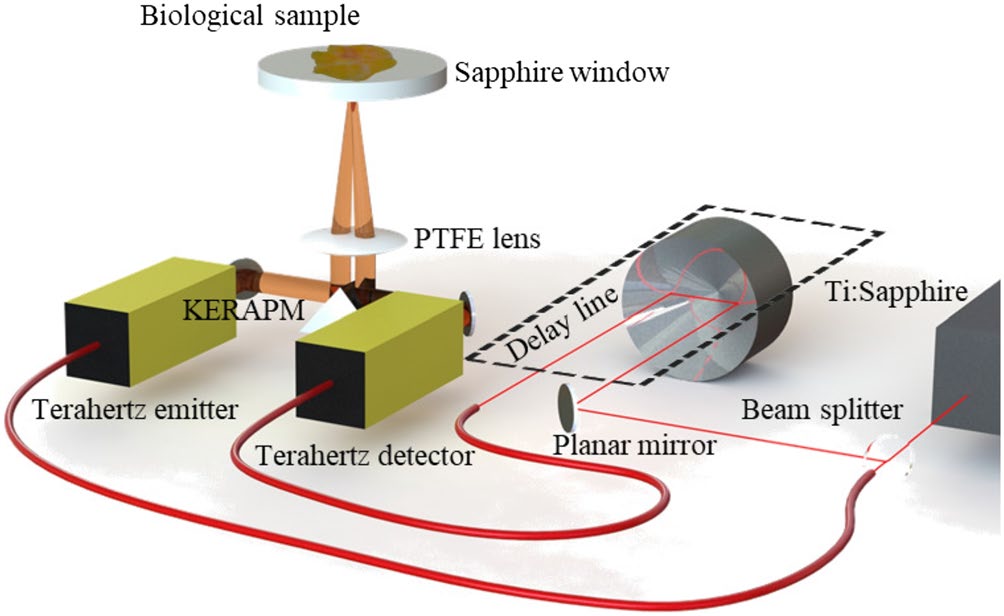
A TeraView TPS3000 time-domain system operated in reflection from 200 GHz to 2 THz. Broadband pulses from a GaAs photoconductive antenna were focused onto tissue supported by sapphire, and the returning field was coherently detected in a nitrogen-purged enclosure. A metal reflector in the holder supplied the reference response. For every image pixel, the authors compared the experimental transfer function with modelled responses generated for candidate complex refractive indices. The real index was searched between 1.5 and 3 and the extinction coefficient between 0 and 1, with the sapphire properties fixed. The classification analysis used the recovered real index at 550 GHz, selected to balance tissue contrast and signal-to-noise ratio.
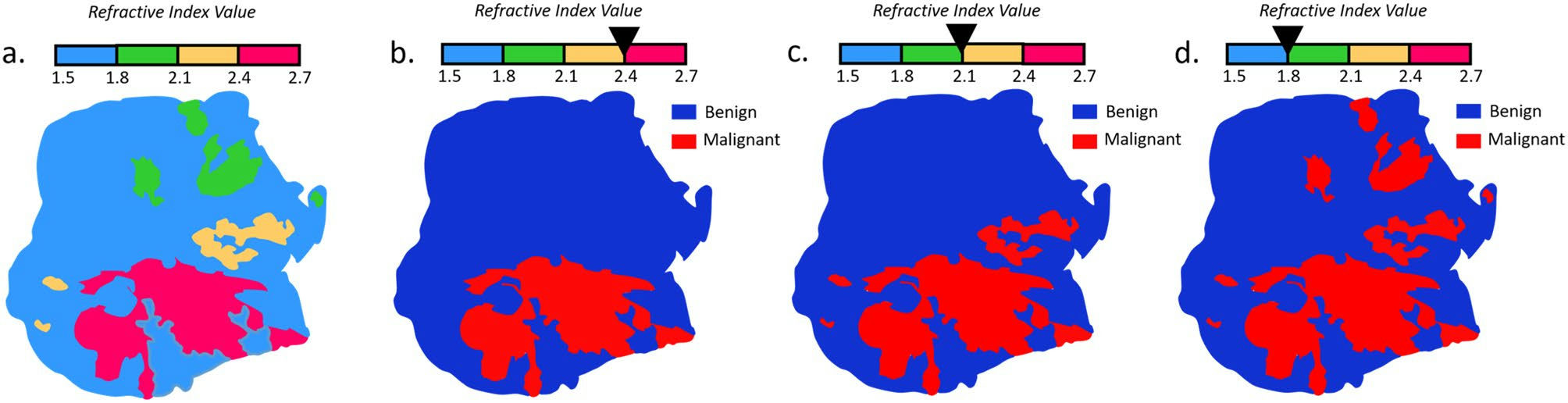
Pixels above a chosen index threshold were initially marked malignant. The team then applied three structuring elements of increasing width, labelled phi1 to phi3, alongside the undilated phi0 case. Dilation was confined to the tissue contour, preventing the binary mask from growing into the surrounding background. A larger element fills wider gaps and increases the area classified as tumour. Threshold and element size were varied together because they exert opposing effects: a high threshold selects fewer, more strongly contrasting pixels, while a wide dilation spreads those selected points over a larger neighbourhood.
Comparison with pathology required the two image spaces to be aligned. The researchers extracted each specimen contour, rescaled it using bicubic interpolation and iteratively rotated it to maximize the Pearson correlation between outlines. Confusion matrices and receiver-operating-characteristic curves were then calculated over the registered pixels. This procedure is transparent and reproducible, but it does not remove deformation between fresh tissue and the processed histology section. A slight mismatch at a convoluted boundary may count as many false positives or false negatives even when the terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More contrast is spatially close to the pathological region.
Uneven results across three carcinoma specimens
For the first invasive ductal carcinoma, a relatively high refractive-index threshold, around 2.5 to 2.6, combined with the largest structuring element gave the most favourable balance: sensitivity approached 80% and specificity 82%, with an area under the ROC curve around 0.83 to 0.84. The second ductal specimen reached a similar sensitivity of roughly 78% but specificity fell to about 57% in the reported best dilated configuration. These differences show that dilation can recover positive area while also incorporating substantial benign tissue. They caution against presenting the strongest single result as the performance of the method as a whole.
The invasive lobular carcinoma was more difficult. Its best reported configuration, using the largest element near a threshold of 2.3, produced sensitivity around 53%, specificity around 76% and an AUC of approximately 0.67. Lobular carcinoma can infiltrate as a more dispersed population of cells than the denser regions encountered in ductal lesions. Such morphology weakens the assumption that a compact expansion around high-index pixels will reproduce the pathological extent. Registration error and small local differences in hydration may further influence the result.
Several modelling choices also delimit the evidence. The classifier used one frequency rather than the complete spectral waveform. Although the inverse calculation included a complex index search, the tissue discrimination focused on the real component and assumed limited value in extinction-coefficient differences. The dilation shape and width were hand-defined, not learned on an independent training set. Most importantly, three specimens cannot characterize inter-patient variation or support a prospective estimate of diagnostic accuracy. The results are a comparison of processing configurations within a pilot data set.
The paper’s useful insight is that physical contrast and spatial context need not be treated separately. A refractive-index estimate gives the binary mask a measurable electromagnetic basis, while morphology encodes the expectation that tumour-associated contrast may extend around a detected point. Future research could test that idea on larger, blinded collections, preserve three-dimensional correspondence between measured tissue and histology, use multiple frequencies and compare dilation with other segmentation approaches. Validation would also need predefined thresholds rather than optimization on the same specimens used for evaluation.
This collaboration spans pathology, terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More spectroscopy, semiconductor electronics and image analysis. It presents a plausible supporting method for research on excised tissue, not a surgical decision tool. Under the reported conditions, a broad structuring element improved classification for selected ductal specimens, while the weaker lobular result exposed the sensitivity of the approach to tissue architecture. That contrast between success and limitation is central to the article: morphological processing can redistribute measured evidence, but it cannot create biological specificity that the underlying measurement and sample set do not contain.
Bibliographic reference
Recommended citation: Cassar, Q., Caravera, S., MacGrogan, G., Bücher, T., Hillger, P., Pfeiffer, U., Zimmer, T., Guillet, J.-P., & Mounaix, P. (2021). TerahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More refractive index-based morphological dilation for breast carcinoma delineation. Scientific Reports, 11(1). https://doi.org/10.1038/s41598-021-85853-8
Publisher: Springer Science and Business Media LLC. Airtable record: reccogBDSh6d6PtB1.