Research publication · Ex vivo terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More near-field microscopy
Scanning point terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More source microscopy of unstained comedo ductal carcinoma in situ
Comedo ductal carcinoma in situ has a recognizable architecture: viable neoplastic cells form a dense rim around a central zone of necrotic material. Those structures can be only hundreds of micrometres across and are therefore blurred by conventional far-field terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More systems. In this study, a scanning point terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More source microscope maps an unstained, formalin-fixed and paraffin-embedded human breast section containing a comedo-DCIS lesion. Transmission and reflection images distinguish the dense peripheral neoplasm from a necrotic core about 500 micrometres in diameter and from surrounding fibrous tissue. The result is a single-specimen ex vivo demonstration of morphology-related contrast; it is not evidence of clinical diagnostic accuracy or readiness for surgical use.
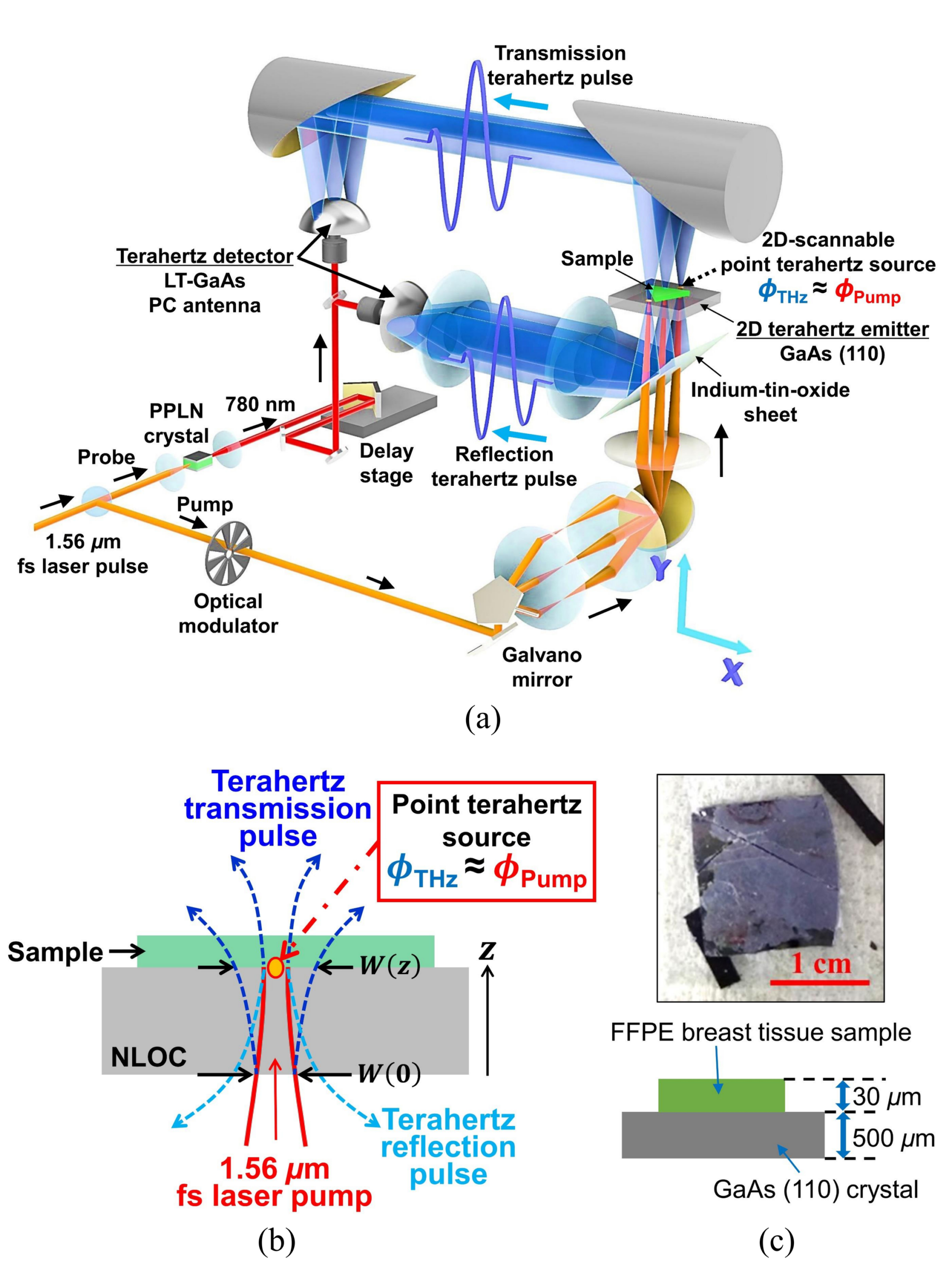
The SPoTS microscope creates radiation immediately beside the sample instead of focusing a free-space terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More beam to a diffraction-limited spot. A 1.56 micrometre femtosecond fibre laser is split into pump and probe paths. The focused pump generates a local broadband terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More pulse by optical rectification in a 500 micrometre, (110)-oriented GaAs plate. The tissue rests directly on that plate, within the localized field. A galvanometer scans the optical focus, and a photoconductive antenna records the outgoing waveform using a synchronized probe. This probe-free arrangement avoids dragging a metallic near-field tip across the section and provides spatial resolution around 10 micrometres under the reported conditions.
The human specimen was processed by routine fixation and paraffin embedding, then sectioned to approximately 30 micrometres and mounted on GaAs. Histology from the same pathological material identified the neoplastic rim, central comedo necrosis and adjacent fibrous tissue. Embedding makes the thin sample mechanically stable and largely removes free water and lipids, which helps expose structural differences. It also changes the dielectric environment. The contrast observed here must therefore be attributed to the prepared section and cannot be numerically transferred to fresh tissue without a dedicated comparison.
Featured visual: Image 1 from the Airtable record associated with this publication. Consult the original paper for the authoritative figure caption and interpretation. Source publication.
Visuals are drawn from the Airtable research archive. Figure numbering, rights and interpretation should be checked against the original publication before republication outside this site.
Resolving the rim and necrotic core in two geometries
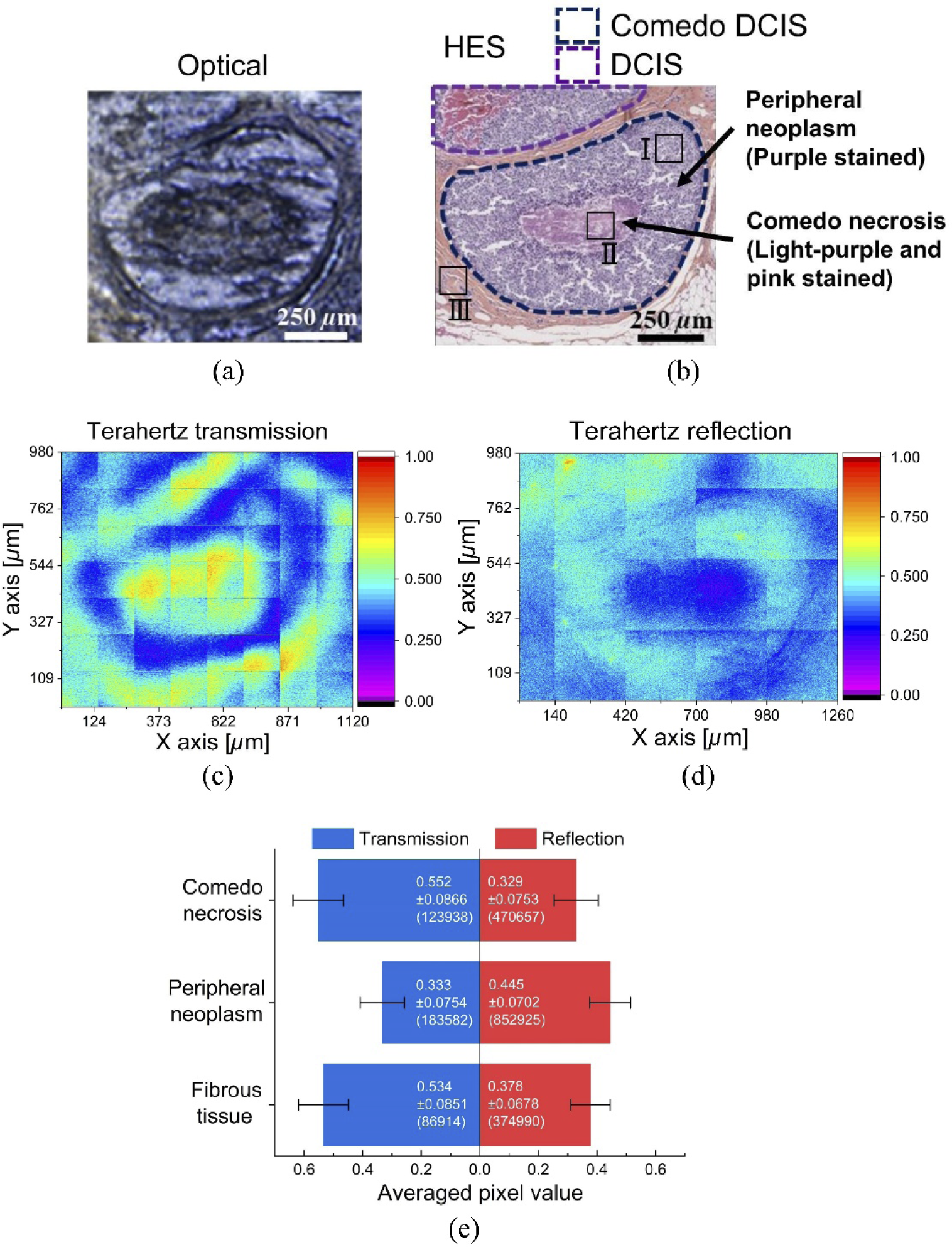
The time-domain acquisition covered an 8 ps window, supporting spectra to roughly 4 THz in transmission and 2.5 THz in reflection. The local field was scanned over 280 by 280 micrometre tiles, which were assembled to cover the larger lesion. In transmission, the dense peripheral neoplasm attenuated the field most strongly. The central necrotic region produced the highest transmitted amplitude, while fibrous tissue lay between them. The lesion’s ring-like organization was visible because the near-field source resolved features much smaller than the free-space terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More wavelength.
Reflection reversed the ordering of the main signal amplitudes. The neoplastic rim returned the strongest field, fibrous tissue was intermediate and necrosis was weakest. Average pixel values were calculated for the three annotated regions rather than relying only on visual colour scales. Time traces supported the same ordering, and normalized spectra showed broad differences across approximately 0.5 to 2.5 THz. No narrow, tissue-specific absorption resonance was established. The maps are thus best explained by combined changes in effective refractive index, attenuation and interface response.
High-magnification pathology provides a plausible structural basis. The peripheral rim contains densely packed nuclei, the core contains necrotic material with far fewer intact nuclei, and the fibrous region has a sparser cellular distribution. Nucleic-acid-rich nuclei and cellular packing alter the local dielectric properties, so a cell-dense area can attenuate and reflect differently from necrosis. The experiment shows a correlation between this architecture and the terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More measurements. It does not isolate nuclear density from every other variable, including section thickness, residual paraffin, extracellular matrix and small registration differences.
A morphology experiment, not a clinical test
The main advance over earlier far-field work is the ability to observe internal organization within one small DCIS lesion. Merely detecting that a region differs from fibrous tissue would not distinguish comedo morphology; resolving its lower-density centre and higher-density rim provides more specific spatial information. The acquisition is label-free in the sense that no stain was required to produce the terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More contrast. Histological staining remained indispensable for identifying the structures and evaluating what the map represented.
Several limits prevent a clinical interpretation. The evidence derives from one prepared specimen, so no sensitivity, specificity or generalization across DCIS subtypes can be estimated. A thin dehydrated section is very different from an irregular, water-rich surgical surface. The field of view is small and larger maps require stitching, while close placement on the emitter constrains sample handling. Acquisition speed and signal-to-noise must also be considered together: reducing integration can accelerate a map but may obscure subtle regional differences.
Future studies could repeat the protocol across multiple lesions and benign ductal structures, use blinded pathology annotations and quantify the reproducibility of regional amplitudes. Measuring adjacent sections at controlled stages of hydration would help separate cellular architecture from water content. For fresh tissue, reflection is the more plausible geometry, but it would require robust contact control or a defined near-field gap and a strategy for uneven surfaces. None of those validations is supplied by the present article.
The paper nevertheless provides a valuable test of scale. It shows that broadband terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More contrast can follow a roughly 500 micrometre necrotic core within a larger comedo-DCIS architecture when the source is localized to about 10 micrometres. That is a physical imaging result with relevance to tissue research, not a claim that comedo-DCIS can be diagnosed automatically. By pairing near-field engineering with pathological interpretation, the collaboration establishes a platform for investigating which microscopic features contribute to terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More response.
Careful follow-up could also combine the terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More map with optical or other microscopic modalities, not to replace the reference method but to identify complementary contrast. The most defensible present conclusion is narrow: under the stated ex vivo preparation, the SPoTS microscope distinguished neoplastic rim, comedo necrosis and fibrous tissue in both transmission and reflection. The size of the observed structures explains why a conventional millimetre-resolution instrument would not have shown the same morphology.
Bibliographic reference
Recommended citation: Okada, K., Cassar, Q., Murakami, H., MacGrogan, G., Guillet, J.-P., Mounaix, P., Tonouchi, M., & Serita, K. (2022). Scanning point terahertzTerahertz radiation is electromagnetic energy commonly associated with frequencies around 0.1 to 10 THz, between microwaves and infrared, where many materials reveal distinctive propagation, absorption, and imaging behavior. More source microscopy of unstained comedo ductal carcinoma in situ. Optics Continuum, 1(3), 527. https://doi.org/10.1364/OPTCON.448444
Publisher: Optica Publishing Group. Airtable record: recLmRHC92S1qS8g3.